
What is the Perfect Embryo?
As an embryologist, I've been asked a lot of questions about embryos. For example, what makes an embryo suitable for transfer? How do embryologists calculate which embryo is best for transfer? And what is the perfect embryo?
These are valid questions that unfortunately require complex answers. Before answering these questions, it's important to review how embryos normally grow and how they are graded.

What is the Perfect Embryo?
Disclaimer: I am not a medical doctor. Please always discuss any health concerns with your doctor before making any decisions about your health.
Normal Embryo Development
Every embryo begins as one cell inside a zona pellucida (shell) when fertilization occurs. Over the next few days, this one cell divides into two cells, which then divides into four cells, and so on. Eventually, these cells clump together to form a ball of cells known as a morula. Around 4 days after insemination, a small cavity (blastocoel) forms inside the morula as it reaches the early blastocyst stage. As the embryo develops into a blastocyst, the cells inside the embryo begin to have different functions (discussed later). The blastocoel quickly grows as the cells continue to divide in the embryo. When the blastocoel takes up 100% of the embryo, it becomes known as a full blastocyst. Eventually, the embryo grows so much in size that the zona thins around the embryo (now known as an expanded blastocyst). As the zona thins, a small hole forms in the zona, and the embryo begins hatching from the zona. This hatching blastocyst then fully hatches from the zona, which is required for the embryo to implant into the uterine lining. Embryos normally begin to hatch around 6 days after insemination occurs.
Embryo Grading
Embryos are graded based on specific physical criteria that allow embryologists to determine which embryos are suitable for transfer. Some clinics grade embryos 3 days after insemination, while other clinics wait until at least 5 days after insemination to begin grading embryos. Though there are slight variations in the way that clinics grade their embryos, most clinics grade embryos based on the following criteria.
Day 3 Grading:
On day 3, embryologists expect embryos to have the following:
1. At least 6 cells (if there are less than 6 cells, cell division is delayed, and the embryo will most likely not grow properly).
2. Less than 10% fragmentation (fragmentation occurs when cell division does not occur properly. Instead of dividing, the cells break into small, unusable fragments).
3. Perfect or moderate cell symmetry (the cells in the embryo are all roughly the same size. If the cells are severely asymmetrical, it could mean that cell division is not occurring properly, and the embryo will likely not grow).
Day 5, 6, and/or 7 Grading
Embryo grading on day 3 does not always determine how an embryo will grow. For example, a good quality embryo on day 3 is not guaranteed to grow into a good quality embryo by day 5. For this reason, many clinics wait until 5, 6, and/or 7 (depending on your clinic's protocol) days after insemination to grade embryos. At this point, embryologists will grade embryos based on 3 criteria:
1. Their stage of development. Many clinics utilize a numeric system known as the Gardner scale to grade their embryos. See Table 1 for more information about how the Gardner scale is used to grade embryos. Other clinics may utilize other systems to determine an embryo's stage of development. By day 5, embryos are expected to at least be at the early blastocyst stage of development.

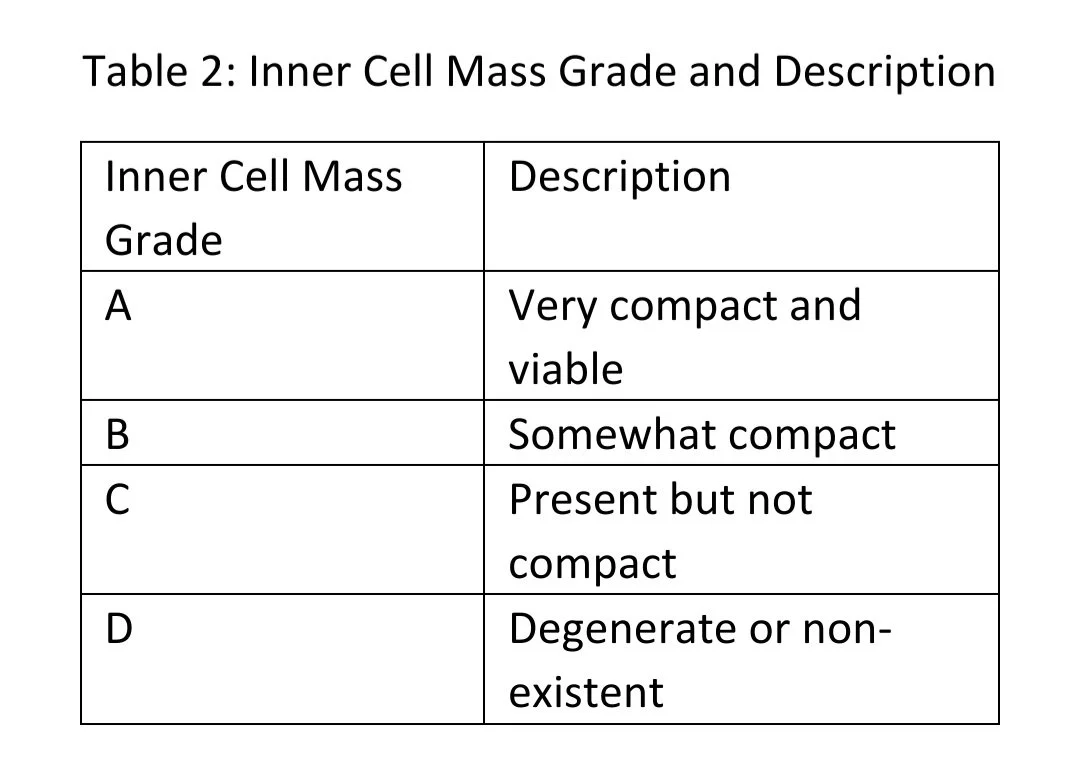
2. The inner cell mass (ICM). The ICM refers to the group of cells that eventually develop into the fetus (baby). Many clinics grade an embryo's ICM using an A, B, C, and sometimes D scale, with A being the best grade. See Table 2 for more information about how the ICM is graded, keeping in mind that each clinic may have their own system in place for grading an embryo's ICM.
3. The trophectoderm (TE). The TE refers to the cells that line the embryo's shell and eventually develop into the placenta. Like the ICM, many clinics also grade an embryo's TE on an A, B, C, and sometimes D scale, with A being the best. See Table 3 for more information about how the TE is graded, keeping in mind that each clinic may have their own system in place for grading an embryo's TE.

One important note: embryo grading can help determine an embryo's potential success rate. However, embryo grading is subjective, meaning that it may change from person to person. Therefore, embryo grading is not a definitive way to determine an embryo's success rate, but rather one variable to consider when calculating success rates.
Preimplantation genetic testing (PGT)
Another important factor to consider when determining if an embryo is suitable for transfer, is its genetic composition. Briefly, all of the cells in our bodies should contain 2 sets of 23 chromosomes (which contain the cell's DNA), and embryonic cells are no different. One set of an embryo's chromosomes derives from the egg and the other set derives from the sperm. These chromosomes replicate during cell division, so the new cells should have the same number of chromosomes as the parent cells.
However, it's possible for an egg, sperm, and/or embryo to have an abnormal number of chromosomes. These abnormalities may cause embryos to have genetic diseases such as Turner Syndrome, Downs Syndrome, and Klinefelter's Syndrome. Preimplantation genetic testing (PGT) is a screening test that can help determine whether or not an embryo contains the correct number of chromosomes. I will briefly discuss the concept and process of PGT, but keep in mind that there is a lot more information regarding PGT than what I discuss here.
PGT can be performed on an embryo by testing the chromosome numbers from 5-10 of the embryo's cells (which are obtained through an embryo biopsy). The DNA in these cells is then amplified (a lot of copies are made) and run through a machine that analyzes the DNA in these cells. If a specific percent of the cells in the biopsy sample are chromosomally abnormal, the embryo is considered abnormal (aneuploid) and is not recommended for transfer because:
1. Aneuploid embryos have a very low chance of implanting
2. Aneuploid embryos have a very high chance of miscarrying
3. Aneuploid embryos have a very high chance of resulting in preterm delivery and/or birth defects
Again, there is a lot more information available about PGT. However, it's important to note that its PGT results are a more definitive way to determine an embryo's success rate than its grade.
Determining which embryos are suitable for transfer
The goal of any embryo is to ultimately be transferred. However, only certain embryos are "usable" (able to be transferred, frozen, and/or biopsied).
So, what makes an embryo usable? Keep in mind that each clinic may have their own protocol for determining if embryos are usable, so talk with your clinic about their particular protocol if you have questions about it. At the end of the day, usable embryos should have certain characteristics that statistically increase their likelihood of achieving healthy pregnancies. In other words, embryos that do not have a high chance of achieving healthy pregnancies are usually discarded.
When it comes to embryo grading, there are a few things that make them usable:
1. Embryos that are transferred on day 3 (this is becoming less common) should have more than 6 cells, less than 10% fragmentation, and perfect/moderate cell symmetry. Embryos that are not at these stages may also implant, but their success rates are significantly lower.
2. Most clinics transfer/freeze/biopsy embryos on days 5, 6, and sometimes 7. On these days, usable embryos are usually at the expanded, hatching, or fully hatched stage of development. Embryos that are not at these stages may also implant, but their success rates are significantly lower. Further, usable embryos on these days usually have an ICM and TE grade of A, B, and sometimes C (this also varies between clinics). For example, an embryo that is hatching with an ICM grade of B and a TE grade of A would be usable.
Determining the best embryo for transfer
If multiple (normal, if tested) embryos are usable on the same day, embryo grading can help determine which embryo(s) is the best option for transfer. Embryos that have higher ICM and TE grades are often transferred before embryos with lower ICM and TE grades. For example, a 5AB will likely be transferred over a 5BB.
What is the perfect embryo?
So, we now know how embryos normally develop and how they are graded. With this set of information, we can fully understand what would make an embryo "perfect."
Let's start with a day 3 embryo. The perfect day 3 embryo would consist of:
1. 8 or more cells
2. 0% fragmentation
3. Perfect cell symmetry
Now let's look at the perfect day 5 embryo. This (genetically normal) embryo would consist of:
1. An expanded blastocyst stage of development
2. A compact, perfect (grade A) inner cell mass
3. A full, uniform (grade A) trophectoderm
On days 6 or 7, the perfect (genetically normal) embryo would consist of:
1. Either a hatching or fully hatched stage of development
2. A compact, perfect (grade A) inner cell mass
3. A full, uniform (grade A) trophectoderm
A final note
Don't get discouraged if your embryo is not "perfect." In fact, most embryos that are transferred are not AA quality, and these embryos still result in healthy pregnancies. Like us, each embryo is different and, in my opinion, perfect in its own way.

My name is Jessica and I am the voice behind Explaining IVF. I obtained my Master of Biomedical Science at Colorado State University and have been an embryologist since 2018. My favorite part of being an embryologist is helping people build their families. I started Explaining IVF to educate people about IVF and infertility so they can make informed decisions about their treatments and optimize their results. In my free time, I enjoy traveling, reading, and spending time with my friends and family.
Website: www.ExplainingIVF.com
Medical Disclaimer:
The information provided in this blog is intended for general informational purposes only and should not be considered as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your healthcare provider or qualified medical professional with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this blog.